Tongue, Lips and Cheek Ties also known as TOT (Tethered Oral Tissues)
By Beverly Morgan, IBCLC, FILCA
first published in 2013, last revised 1/2019
first published in 2013, last revised 1/2019
|
Tongue ties (attaching to lips and cheek or inside the tongue causing flexibility issues) can add another level of challenge to breastfeeding as they disrupt the normal function of the oral cavity as well as swallowing. Many MOBI mothers ultimately discovered that a variety of their breastfeeding problems were related to TOT (also called tight frenulum’s or Ankyloglossia or tongue ties) after initially being told their child was not tongue tied. They may have been told it was a mild tie and would not cause breastfeeding problems. Or perhaps tongue tie or other ties were not addressed at all.
|

|
The tongue is supposed to separate from the floor of the mouth in utero, for some people the separation is not complete causing a tongue tie which interferes with effective tongue movement and causes restriction to muscles connected to the tongue. TOT are among the most common cause of breastfeeding difficulties, however they are often under-diagnosed or dismissed as “not a problem”. Issues such as sore nipples, poor breast drainage, low milk supply, for mother, low weight gain, long feeds, poor feeders or difficulty swallowing, pushing out the nipple, and shallow latch, may be related to TOT. It is important to remember that breastfeeding is complex, one or two check marks on this list does not necessarily point to tight frenulum’s; there may be other issues at play. See an Internationally Board Certified Lactation Consultant (IBCLC) to help you navigate the rough waters if you are having breastfeeding challenges. The mothers here on MOBI can also give you practical advice and emotional support.
Breast Related Challenges for Mom
- Sore Nipple tips-- as the tender nipple is forcefully pinched inside the baby’s mouth during feeding (lipstick-shaped nipples blanched and sore after nursing or a white seam across the nipple)
- Abrasions on the underside of the nipples/areola-- (mothers report it feels like sandpaper), as the baby tries to stretch his tongue to hold the nipple. As the tongue is fatigued, it slides back, causing rubbing on moms skin.
- Sore areola-- as the baby clamps with his gums to help hold the breast in place or as he clamps and releases to get milk to flow. (mother’s often call this baby stapler, or baby jaws)
- Mastitis-- as the breast does not drain evenly because there is pressure on breast/areola/nipple that blocks flow from an area of the breasts
- Diminishing milk supply— when the milk is not removed well, either because of pressure on the breast from incorrect sucking patterns or from the baby’s inability to transfer milk well
Breastfeeding Issues that Implicate Tongue Tie
Parents looking for reassurance that they are doing the right thing can take comfort at looking at a list of common symptoms associated with lip and tongue tie. If mother is not experiencing problems with breast pain or milk supply issues and baby is not experiencing situations like the ones listed below then it is time to look for other reasons if there is still concern. Not all breastfeeding problems are caused by tongue and lip tie.
- Long feedings, with poor milk removal uses energy reserves but does not provide the amount of milk needed and results in poor weight gain
- A baby that falls asleep after the first letdown or as soon as he gets to breasts – is signaling that he is not receiving milk fast enough to keep him engaged, or too fast and he gives up.
- A baby that fusses at the breast indicates a baby that is finding breastfeeding challenging, or uncomfortable
- Clicking during feedings often happens when baby can’t maintain suction or when he is receiving milk to quickly for his swallow
- Cheeks or edge of mouth sucked in indicates poor muscle tone and tongue placement
- A baby that does not open his mouth wide. (Restriction may be causing the baby to avoid opening wider, it may be that a lip tie is impeding the full mouth opening.
- A baby that does not maintain a latch well (either sliding off the breast, rubbing with his tongue, milk leaks from his mouth because of a poor seal,
- A baby that gags easily is often a baby that cannot move his tongue effectively
- When a baby can’t swallow efficiently it leads to milk being drawn into the ear canals or into the baby’s lungs.
- A baby with a high palate-- in utero the tongue sweeps across the palate, causing it to widen and flatten ,the breast fits better into a broad pallet than a high arched one, later the growing child will have room for his teeth, .however when the tongue is tied, this is not always possible
- A baby that pushes the nipple out of his mouth rather than drawing it in is not moving his tongue correctly, often it is because it is pinned or tied down...
- A baby that does not open his mouth well is responding to his physical limitations
- Baby teeth marks on the breasts once teeth come in if the baby has used his jaws to help stabilize the breasts.
- Hiccoughs after feeding as he has not been able to pace his breathing well during feedings
- Soiled diapers that do not have much solid content - would suggest that baby is receiving more foremilk (skimmed milk) than hindmilk (cream) a common problem with poor suction or milk removal.
Below you can see a couple of pictures of a tongue-tied baby:

|

|
Other Indicators a Baby May Have TOT Restrictions
- A baby that needs to be taught to bottle feed, or appears to be “a greedy eater”. He in effect may be trying to swallow rapidly to allow for breathing
- A baby with frequent sinus or ear infections or with fluid in their lungs
- A baby with difficulty with mouth closure resulting in mouth breathing
- Noisy breathing/ snoring, sleep apnea
- A baby who will suck and chew at foods then spit it out rather than swallow it.
- A baby who needs to be held upright for comfort or to ease breathing and/or gas for tummy relief
- A restless baby who has difficulty sleeping and wakes frequently wanting to feed again
- A child with constipation, as where there is restriction on the mouth end, there is often restriction on the anal end.
- A baby with reflux or painful gas
- An “in arms baby” who fusses when not held upright for comfort or to ease breathing and/or gas for tummy relief
Parents struggle with the decision of whether to release the restriction or to take a wait and see position, especially if those around them dismiss the restrictions as unimportant. Baby and mother may have learned compensations as a get-around to correct function. Baby may be gaining weight well for example, but may hurt mom’s nipple. He may be a noisy breather and choke easily, but a mom may not have made a connection between the dysfunction caused by the TOT and his swallow or breathe issues. He may not drain the breast well but moms need to compress the breasts for good drainage or her lowered supply or frequent blocked ducts or breast infections may not be seen as having any connection to the compromised function caused by oral tethers.
Massage for Releasing Tension in Muscles Before and After the Release
Providers differ on whether any aftercare is needed to keep the release from healing back together but using gentle massage once the restriction is found is becoming a more common practice. The tie cause tight muscles and gently massaging the cheeks and in the baby's mouth can help relax the muscles. It also prepares the child for aftercare when the massage is already a comfortable and welcomed routine, not a new routine introduced after the release. Be sure to smile and make it a game. If baby is fussy at the moment try again later.
Incorporate a gentle massage on tongue and cheeks and lips to help the support structure that has been restricted
Try this on your own face to get a feeling for what feels good to you.
- Cheeks: Massage the cheeks using your hands lightly move the skin of the cheeks in a circular motion; you may notice that this feels good to your ears too.
- Nose: Place one finger on each side of the bridge of the nose and lightly stroke towards the ears. Place one finger below the nose and stroke down towards the upper lip. Stroke from the center of the upper lip to each side in the mustache area as if you were smoothing a mustache.
- Chin: Placing one hand on the chin, massage in a circular motion then with 2 fingers of both hands on the chin stroke form the center of the chin to the sides, as if you were applying makeup to your face. Sweep your fingers from the neck to the bottom of the chin.
- Jaw line: Place your fingers just under your ears and drag them gently down to meet at your chin.
- Neck: Place your hand on the side of the neck and do circular motions as you might if you had tight muscles in your neck
- Mouth: Lift the upper lip (gently especially when the restriction is tight and painful) and lightly stroke the gums area, Lift the lower lip gently out and stroke the gums and inside of the lip. Lift the tongue and massage on the underside of the tongue and the floor of the mouth. Massage gently along the sides of the tongue. Massage on the top of the tongue , starting at the tip using your finger pad to make little circles on the tongue, go as far back as you can without causing a gag. If a gag is triggered move the finger slightly towards the front of the tongue and stop movement. Once the person is comfortable resume the circular motions where your finger is. The goal is to be able to go further back and be ready to desensitize the tongue after the release is done. A sensitive gag is a byproduct of the tethered tongue.
- Tummy Time is an important to the overall growth of the baby and has added advantages after the release. With "Back to Sleep" being such a large part of a baby's day there is not as much movement to the neck/shoulders area and the tongue is more likely to stay in a lowered position that the muscle memory dictates. Encouraging play that involves lifting the head and upper body encourages the tongue to lift from the floor of the mouth and strengthening the muscles in the throat, neck, and upper body.
Many mothers find The Nurtured Child's approach to be helpful.
- Before starting the stretching exercises, make sure that your hands are clean and your nails are short to avoid accidentally hurting your baby. I suggest that clean hands are better than gloved hands.
- To stretch the lip. you want to pull the lip out and up towards your baby’s nose, applying gentle pressure to expose the area where the release was made
- For the tongue, most parents find it easiest to position baby on their back with their head towards you and feet pointing away from you.
- Use your index fingers to get under your baby’s tongue and elevate it so that the area where the restriction or release site is exposed. After the release hold the stretch for 3-5 seconds, position your fingers on either side of the diamond shape where the release was made, and pull your finger apart for 3-5 seconds to stretch the surgical site horizontally.
- Many parents do the stretching from 3 to 6 times in 24 hours, including at least one stretching session overnight.
- Stretches should be quick, you only need to hold them for 3-5 seconds.
- Many parents wait up to 24 hours before adding in gentle massage of the surgical sites, done for a few seconds after the stretches. If stitches are used providers will generally tell parents to wait until after the stitches have dissolved to do stretches.
- If your provider does not give you a timeline for doing the exercises continued for at least 7-10 days after the procedure . For some babies healing may take a little longer, so if you stop the stretches and breastfeeding becomes uncomfortable again, then start the exercises again and continue for another week. (C. Watson Genna, personal communication, June 17, 2011)”
http://nurturedchild.ca/index.php/breastfeeding/challenges/what-to-expect-after-tongue-tie-and-lip-tie-release/
If the child is always distressed by having touch around the mouth rather than finding it pleasant you can self refer to a early childhood intervention program in your area.
- With an older child you can use a mirror so the person can see what the tongue is doing. Use a mirror and have the person look at the areas where the tie was released. The tongue will stretch as the person lifts the tongue to look at the released area.
- When sticking out the tongue out try to think to PUSH OUT rather than STICK OUT the tongue.
- Teach him to do the little circles on his tongue that actually feels good when you know you do not need to do it in the gag area.
- Put nut butter or other yummy food that has some mass on the person’s lips in the area you want him/her to reach. Let the person watch as he tries to lick it off.
- Use a cheerio's type food that softens in the mouth to see if he can hold it with his tongue against the arch of the palate to encourage lift. It melts well and is too small for choking. As we learn more about what may cause the regrowth of filaments, there is a theory that sugar has a possible impact on healing and filament formation of frenectomy sites so avoiding sweet foods for now seems a very good practice.
- Teach him to do the little circles on his tongue that actually feels good when you know you do not need to do it in the gag area.
- Use a toy such as an Oball shaker rattle that encourages a baby to use his tongue to explore the angles of the toy. That can help a child exercise using their tongue.
|
Video: Frenotomy Assessment
Hazelbaker score assessment for the treatment of Ankyloglossia or tongue-tie. |
|
|
Video: Dr. Kotlow Shows How to Examine and Infant for Tongue Tie
In this video, Dr. Kotlow shows how to identify a tongue tie in an infant. |
|
The Difficulties Do Not Stop when Breastfeeding Stops
I am an IBCLC and I did not realize I was tongue tied until I was 67 years old as I was putting together the information on adult tongue ties. I had my tongue and lower lip tie released. I am glad I did. In my case I went to Dr. Stacy V. Cole in Fort Worth, TX. I urge every parent who has a tongue tied baby to have the trusted provider also take a look at their lips/tongue. If you can have it released at the same visit as the child, even better! I can say the laser release was less painful than having bone grafts, implants, root canals, and extractions and filling that I have had because of the tongue and lip ties. The constant ear infections I had as a child until I finally lost my tonsils and adenoids were very uncomfortable too. I remember the years of ear infections and ear aches and tooth aches, common things for tongue tied people. Thankfully I have not had TMJ, teeth grinding, or headaches, and these are the tip of the iceberg.
Many of the issues that caused problems for the baby cause problems for the adult, constipation, reflux, mouth breathing/ snoring, sleep apnea, headaches, sore tired mouth, teeth grinding, neck and back pain, plague people with oral dysfunction. Many parents do not recognize that some of the chronic issues plaging them are related to tethered oral tissue until they learn more about the condition.
For parents struggling to make a decision for non-nursing infants and older children or for themselves, especially where they are hearing opposing views, the following list can help..
Below you can see a few pictures of my tongue and lower lip before and after the surgery:
Many of the issues that caused problems for the baby cause problems for the adult, constipation, reflux, mouth breathing/ snoring, sleep apnea, headaches, sore tired mouth, teeth grinding, neck and back pain, plague people with oral dysfunction. Many parents do not recognize that some of the chronic issues plaging them are related to tethered oral tissue until they learn more about the condition.
For parents struggling to make a decision for non-nursing infants and older children or for themselves, especially where they are hearing opposing views, the following list can help..
- Mouth Breathing (there are other causes such as allergies) “Common symptoms of mouth breathing include dry, cracked lips, a dry mouth, bad breath, snoring and daytime fatigue., mouth breathing can cause gingivitis and increase the risk of developing serious cardiovascular conditions. It limits the amount of oxygen in the blood, increasing your likelihood of having high blood pressure and heart complications. The poor sleep associated with mouth breathing also reduces cognitive function and energy level during the day. …Dry mouth can lead to the development of long-face syndrome, a condition characterized by a long, narrow face, crooked teeth and a narrow mouth” according to dentist Dr. Yosh Jefferson in Know Your Teeth, an Academy of General Dentistry website.: http://www.livestrong.com/article/350758-symptoms-mouth-breathing/#ixzz2hueHNgir retrieved 10/16/13
- Sleep impacted by tongue tie is aerophagia, also called aerophagy, -- this is a condition where patients swallow too much air. This air then goes directly to the stomach which can result in a number of complications such as belching, feelings of bloating reflux, gas and/or abdominal pain.
- Dental problems--, if the tongue is not placed correctly in the mouth the shape of the oral cavity are changed. The heavy tongue resting on the teeth will keep them from erupting well. The tongue should be able to rest in the palate protecting the tonsils and helping to support the head and neck. Among other ways the body is impacted a thick, tight superior labial frenulum often results in a space between the front teeth, however the frenlum may be buried above the eruption line so close front teeth does not necessary mean no ties. With a tight anterior labial frenulum or cheek ties the pressure for the tight frenulum may result in receding gums.
- A tight frenulum pulls back on the lower jaw causing misalignment of the teeth, contributing to mouth breathing, to poor mouth closure and impacts oral function.
- Tooth Decay can be caused by crowded teeth making it difficult to floss, dry mouth and by the inability to clear food from the teeth as well as in reaching areas of the mouth where food may be trapped.
- Tonsils can be impacted by dryness causing enlarged tonsils which interferes with breathing and often results in removal of the tonsils, the first area of protection for inhaled germs and allergens.
- Frequent sinus infections as the high arch of the palate compresses the space available for the sinuses
- Difficulty swallowing can cause a person to limit the foods they take to those that can be easily swallowed. In extreme cases, young babies are put on feeding tubes if their swallow difficulties are severe.
- Headaches or TMJ (temporomandibular joint disorder) the joint that connects the jaw to the skull can be impacted by the restrictions caused by tongue/lip ties
- Teeth grinding can be caused by pressure
- A tendency to have inflamed gums, and increased need for fillings and extractions
- Sensitivity about personal appearance
- A “small” mouth
- Tongue tie in the elderly often makes it difficult to keep a denture in place or cause pain as the denture presses against the frenulum.
- Unclear Speech--- with unclear speech a person often feels self-conscious, shy or awkward in new situations, it may impact the type of profession a person chooses
- Stiffness on one side of the body and/or one leg may be smaller in circumference.
Below you can see a few pictures of my tongue and lower lip before and after the surgery:
People share their personal stories about tie release in the sections What We Have Learned From Our Tongue Tied Babies and explores Does it Hurt to Have Ties Released? and Other Frequently Asked Questions .

In order to touch the roof of the mouth with the tongue this is as wide as the mouth could open, notice one of the front top teeth has shifted to cover another tooth. Notice a bottom tooth is tilted towards the inside of the moouth. Notice there is guite a large amount of saliva in the mouth. There is a dark line that shows the groove on the underside of the tongue by the frenulum being pulled tight. Notice the horizontal line caused on the tight upper frenulum above the top lip.
|

The tongue tie 24 hours after release. The tongue could not yet reach the roof of the mouth, but the lift was much better after the release, note
the deep pull linse that go from the nose to the chin. The strong pull liness of the frenlum is no longer on the tongue as it lifts. |

24 hours after the release of the lower lip tie
|

Notice 4 days after release, it is still difficult to stick the tongue straight out. Notice the top lip is turned down holding the tongue out.
|

10 days after release, notice much less saliva in the mouth now. What you can't see is the the salivary glands are not as large now that the constan pull of the tongue tie has been released. The deep fold lines from nose to chin are visible.
|

12 days after the release, it does not take as much effort to push the tongue out off the mouth, notice the lips are no longer needed to hold the tongue out.
|
Classifications of Tongue Tie
All tongue and lip ties do not look the same or cause the same set of difficulties. The classifications into types are to denote position not severity.
Elizabeth V. Coryllos, MD. FAAP, FACS, IBCLC devised a classification system for defining tongue tie that has been widely circulated and adopted. Catherine Watson Genna BS, IBCLC included DR Coryllos definitions in her 2008 book, Supporting Sucking Skills in Breastfeeding Infants (pg. 188)
Type 1 is the attachment of the frenulum to the tip of the tongue, usually in front of the alveolar ridge in the lower lip sulcus.
Type 2 is two- to- four mm behind the tongue tip and attaches on or just behind the alveolar ridge.
Type 3 tongue-tie is the attachment to the mid-tongue and the middle of the floor of the mouth and is usually tighter and less elastic.
Type 4 is essentially against the base of the tongue, and is thick, shiny and very inelastic.
Types 1 and 2, considered “classical” tongue-tie, are the most common and obvious tongue-ties, and probably account for 75% of incidence.
Types 3 and 4 Since they are more difficult to visualize are the most likely to go untreated.
Type 4 is most likely to cause difficulty with bolus handling and swallowing, resulting in more significant symptoms for mother and infant.
- The tongue may be heart shaped
- The person may not be able to raise his tongue to the roof of the mouth
- He/she may not be able to stick the tongue out past the gums or lips.
- He/she may only be able to point the tip of tongue to the chin not straight out of the mouth.
- There may be a crease line in the tongue where it attaches to the floor of the mouth. Look at the cartoon character Sponge Bob, he has the telltale space between his front teeth, that indicates a tight Superior labial frenlum and the crease in his tongue showing it is attached to the floor of his mouth.
Elizabeth V. Coryllos, MD. FAAP, FACS, IBCLC devised a classification system for defining tongue tie that has been widely circulated and adopted. Catherine Watson Genna BS, IBCLC included DR Coryllos definitions in her 2008 book, Supporting Sucking Skills in Breastfeeding Infants (pg. 188)
Type 1 is the attachment of the frenulum to the tip of the tongue, usually in front of the alveolar ridge in the lower lip sulcus.
Type 2 is two- to- four mm behind the tongue tip and attaches on or just behind the alveolar ridge.
Type 3 tongue-tie is the attachment to the mid-tongue and the middle of the floor of the mouth and is usually tighter and less elastic.
Type 4 is essentially against the base of the tongue, and is thick, shiny and very inelastic.
Types 1 and 2, considered “classical” tongue-tie, are the most common and obvious tongue-ties, and probably account for 75% of incidence.
Types 3 and 4 Since they are more difficult to visualize are the most likely to go untreated.
Type 4 is most likely to cause difficulty with bolus handling and swallowing, resulting in more significant symptoms for mother and infant.
Lip Tie
Labial Frenulum Attachment
Superior lip ties (upper lip) are more commonly recognized, but some people also have involvement of the Anterior lip (lower lip) As a person ages the corners of the mouth may be turned down and deep lines on each side of the chin showing the strain of the pull may be visible. Another sign of a lip tie is that when a person smiles or talks only the top teeth are seen
In her book on Sucking Skills, Genna credits Wiessinger, (1995) in identifying the lip frenulum’s impact on breastfeeding. Lip tie may later contribute to receding gums. Bottom teeth may also be turned pushed aside by the lip tie.
In her book on Sucking Skills, Genna credits Wiessinger, (1995) in identifying the lip frenulum’s impact on breastfeeding. Lip tie may later contribute to receding gums. Bottom teeth may also be turned pushed aside by the lip tie.
Classifications of Lip Tie
Lip tie can cause a baby to have a shallow latch and difficulty flanging his lips which can restrict milk flow and can cause sore nipples for mom.
Maxillary Lip-Tie: Dr. L Kotlow introduced a classification system of maxillary lip-tie (Superior Lip-tie) in the article Oral diagnosis of abnormal frenum attachments in neonates and infants: evaluation and treatment of the maxillary and lingual frenum using the Erbium: YAG laser. J Pediatric Dent Care. 2004; 10 (): 11-14 I. The classification is used for infant before the eruption of teeth.
The classification looks at the attachment to the lip and to the maxillary arch.
Class I - The lip can move freely up to the nose, there is no whitening of skin as the frenum is stretched and does not appear to cause problems with breastfeeding.
Class II - There is an insertion point where the free and attached gum/lip tissue but does not go down between the teeth
Class III - This tie holds down the lip and extends down to the area where the central incisors will erupt, but does not wrap round. You will see a small dent, in the area where the two top teeth will be erupting
Class IV - This tie holds down the lip and extends down to wrap into the hard palate just behind the area where the central incisors will erupt. You will likely see that the gum ridge is not smooth or indented but that you can see the tie as it wraps around the gum line.
Buccal Frenulums : Buccal frenulums deserve a mention here. At this time there is no direct connection established between Buccal frenulums and effective breastfeeding however they connect cheek to gum in the cheek area. If all the other attachments are tight ask your provider to release the Buccal frenulums also If the buccal frenulum pulls tightly on the cheeks there is potential for the Buccal frenulums to contribute to Oral Motor Dysfunction. Buccal ties also contribute to deep pockets in the gums.
Maxillary Lip-Tie: Dr. L Kotlow introduced a classification system of maxillary lip-tie (Superior Lip-tie) in the article Oral diagnosis of abnormal frenum attachments in neonates and infants: evaluation and treatment of the maxillary and lingual frenum using the Erbium: YAG laser. J Pediatric Dent Care. 2004; 10 (): 11-14 I. The classification is used for infant before the eruption of teeth.
The classification looks at the attachment to the lip and to the maxillary arch.
Class I - The lip can move freely up to the nose, there is no whitening of skin as the frenum is stretched and does not appear to cause problems with breastfeeding.
Class II - There is an insertion point where the free and attached gum/lip tissue but does not go down between the teeth
Class III - This tie holds down the lip and extends down to the area where the central incisors will erupt, but does not wrap round. You will see a small dent, in the area where the two top teeth will be erupting
Class IV - This tie holds down the lip and extends down to wrap into the hard palate just behind the area where the central incisors will erupt. You will likely see that the gum ridge is not smooth or indented but that you can see the tie as it wraps around the gum line.
Buccal Frenulums : Buccal frenulums deserve a mention here. At this time there is no direct connection established between Buccal frenulums and effective breastfeeding however they connect cheek to gum in the cheek area. If all the other attachments are tight ask your provider to release the Buccal frenulums also If the buccal frenulum pulls tightly on the cheeks there is potential for the Buccal frenulums to contribute to Oral Motor Dysfunction. Buccal ties also contribute to deep pockets in the gums.
Your Release Team
chee If you are looking for confirmation on a suspected tie and/or deciding your child will benefit by having his lip ties and/or tongue tie released carefully consider who will provide the services. Many parents have been mistakenly told there is no concern to find later that indeed there is.
Many providers will say they release tongue ties, but they may deal only with Type I and 2 tongue tie, and not be at all familiar with cheek or lip ties (both top and bottom lip should be checked). Because of the difficulties parents have found finding services, sites such as Facebook Tongue Tie Babies Support Groups have developed for parents and professionals to learn from each other . Many parents have traveled to the providers. If that is not something you can do there are questions you can ask of the person you are considering. The more pre-screening you do the less frustrating it can be.
Questions for the person who is doing the release:
How to find a Frenotomy Surgeon:
- An International Board Certified Lactation Consultant (IBCLC) can help you to protect your milk supply and your breastfeeding relationship. You can think of the IBCLC as the general contractor. You can go to IBLCE.org the certifying body for lactation consultants to find one near you. You can also go to ILCA.org which is the International Lactation Consultant organization to find an IBLC near you. However not all IBCLC's belong to ILCA. or USLC, the US branch.
- A Dentist or Pediatric dentist or an ENT (ear, nose and throat) doctor generally release the more complex tongue ties. Nearly every time there is a lip tie there is also a posterior tongue tie. If the babies difficulties are resolved by a simple tongue tie release you may not need to look further than your local experts. But remember the training commonly available is for releasing only Types 1 and 2. So if the problems are still in play after the recovery period you may need to look for a second opinion
- A myofunctional or myofacial therapist is trained in facial muscles and is invaluable for everyone who is having a TOT release..
- A person who does body work: This might be a chiropractor who works with infants, a massage specialist who does gentle body work such as CranialSacral Therapy (CST). CST is a gentle, hands-on approach that releases tensions deep in the body to relieve pain and dysfunction CranioSacral Therapy - The Upledger Institute www.upledger.com/content.asp?id=61 or a board certified osteopathic physician specializing in Osteopathic/Cranio-sacral Manipulation. Using a holistic approach www.jaoa.org/content/106/2/77.full The person with a tight tie has never had a chance for the muscles to work correctly. Releasing the tongue is the first step. Helping the body to learn how to function correctly is another.
- An occupational therapist, speech-language pathologist, or nutrition advisor will be helpful if there are other challenges
- Optometrist who work in the field of Behavioral Optometrist and vision therapy can teach exercises for correcting eye muscle imbalance or other visual habits that TOT may have imposed.
- Other specialist may also be needed depending on each person’s unique circumstances. As a person's function improves different provider may benefit.
Many providers will say they release tongue ties, but they may deal only with Type I and 2 tongue tie, and not be at all familiar with cheek or lip ties (both top and bottom lip should be checked). Because of the difficulties parents have found finding services, sites such as Facebook Tongue Tie Babies Support Groups have developed for parents and professionals to learn from each other . Many parents have traveled to the providers. If that is not something you can do there are questions you can ask of the person you are considering. The more pre-screening you do the less frustrating it can be.
Questions for the person who is doing the release:
- Ask where she/he was trained for releasing tongue tie
- Ask if anesthesia is required (if it is, keep looking, the child should be awake and able to move his/her tongue, however if you feel it is necessary for your child to have some medication there should be a much better choice than anesthesia.
- Ask if there is an age limit of children (some are comfortable with no medication for newborns, not older children, some are more comfortable with older children and will not do newborns, but will advise waiting.(Look for another provider i this case) Many prefer not to do toddlers as they are strong but not necessary cooperative or willing to listen to instructions. Be guided by your own knowledge of your child and check with providers you trust about your specific needs.
- Ask how many of the tongue ties he/she releases are posterior tongue ties Types 3 and 4. (You will get an idea if the provider knows what you are talking about)
- Ask if lip ties are an additional charge (if they never do lip ties, keep looking)
- Ask if another revision is included in the cost if it is needed
- Ask if they use scissors or lasers (Cold or hot or both) (some excellent providers use scissors some lasers, some combinations of both
- Ask if they have an aftercare protocol and what it is. There is a wide variety from no plan and plans involving many exercises. The important thing is that they have a formulated plan and a rational for the plan they have.
- Ask if parents are allowed in the room if that is important to you, (some very good providers do some don’t). This question is for your comfort.
How to find a Frenotomy Surgeon:
- Academy of Laser Dentistry: http://www.laserdentistry.org/index.cfm/patients/Find%20a%20Dentist
- List of Frenotomy Surgeons (lowmilksupply.org): http://www.lowmilksupply.org/frenotomy.shtml
- Tongue Tie Babies Support Group on Facebook: https://www.facebook.com/groups/tonguetiebabies/
Some people seem to sail through with minimum upset. Others may be very uncomfortable for at least 24 hours.Some are fine on the first days and find by day 3 they are very uncomfortable. If baby has been breastfeeding happily before the release the baby is usually ready to breastfeed as soon as the procedure is over. If he has been frustrated by breastfeeding he may not want to. Even for those who breastfeed well at first later in the day or the second day baby may not want to nurse at all. It is a good plan to have pumped milk available for baby to spoon feed baby if he is not willing to nurse. Mother should also have a pump handy if she is not proficient in hand expressing and baby does not feel like feeding. The first few days are usually the roughest if there is going to be any discomfort. You can take heart in thinking there is a limited amount of recovery pain, the challenges of tongue tie are lifelong.
Your child’s medical care provider will generally direct you in what to use for discomfort. Many providers recommend a pain reliever for the hours (or first few days) to allow baby to feed better and be more comfortable. Once the muscles have been released it may take some time for the baby to learn to use his/her newly freed tongue and with the deeper ties there may be some time where there is some discomfort. Usually much less than is caused by repair of cavities and other procedures, but there may be some unsettled time. Some use homeopathic remedies and or other pain relievers can be helpful in the early hours or days.
Many parents have found that homeopathic Rescue Remedy, a natural remedy created from flower essences; is an effective over-the-counter stress reliever. Many families also use melt-away homeopathic pellets of Hypericum (St. John Wort) or Arnica Homeopathic pellets if you are looking for a homeopathic remedy for pain. Check with your health provider to see if Homeopathic Arnica and St. Johns Wort in pellet form can be used as needed after repair (for a little person you can crush a pellet and add it and add it to a teaspoon of human milk or water.
Your child’s medical care provider will generally direct you in what to use for discomfort. Many providers recommend a pain reliever for the hours (or first few days) to allow baby to feed better and be more comfortable. Once the muscles have been released it may take some time for the baby to learn to use his/her newly freed tongue and with the deeper ties there may be some time where there is some discomfort. Usually much less than is caused by repair of cavities and other procedures, but there may be some unsettled time. Some use homeopathic remedies and or other pain relievers can be helpful in the early hours or days.
Many parents have found that homeopathic Rescue Remedy, a natural remedy created from flower essences; is an effective over-the-counter stress reliever. Many families also use melt-away homeopathic pellets of Hypericum (St. John Wort) or Arnica Homeopathic pellets if you are looking for a homeopathic remedy for pain. Check with your health provider to see if Homeopathic Arnica and St. Johns Wort in pellet form can be used as needed after repair (for a little person you can crush a pellet and add it and add it to a teaspoon of human milk or water.
|
Before

|
After

|
|
Video: Laser Posterior Tongue Tie Revision
Video illustrating a tongue tie revision on a teenager girl. The same procedure is performed on babies, without sedation. |
|
|
Video: Frenuloplasty Procedure
Doctor performing the frenuloplasty procedure with scissors on an infant and assessing the final results. |
|
|
Video: Care after lingual and maxillary lip ties have been revised for breast feeding infants
In this video, Dr. Kotlow explains how to perform post-surgery stretching exercises. |
|
Not All Breastfeeding Problems Are Caused by Tongue-Tie
Guest Post
February 20, 2014
by Bobby Ghaheri, Used with permission
As is the case with the identification of any new medical problem, there is bound to be excitement about helping those in need. Sometimes, that excitement can lead to false attribution of a problem to that "new" diagnosis. While tongue-tie or upper lip-tie are not technically new diagnoses, the correlation between tight frenula and breastfeeding problems is a relatively new one. Because I treat many babies each year where babies are having problems from tight frenula, I inevitably end up turning away many babies who aren't needing treatment.
Not every nail needs the same hammer. Tongue-tie and lip-tie may cause some, but not all, breastfeeding problems.
Not every nail needs the same hammer. Tongue-tie and lip-tie may cause some, but not all, breastfeeding problems.
The first place any mom and baby should go when breastfeeding problems arise is an IBCLC (international board certified lactation consultant). Here is a great post on how to choose a lactation consultant.
There are many potential causes of breastfeeding problems. I asked a group of great lactation consultants for a list of other causes for breastfeeding problems (specifically, pain). Here's what they came up with:
Technique problems - This includes poor latch technique, especially with positioning. Often, inexperienced moms picture breastfeeding like how a baby feeds from a bottle (this can also happen if the baby has nipple confusion when going from a bottle to the breast). They present the nipple instead of the breast, which can cause pain. Poor positioning can certainly be a problem (often caused by the wrong kind of pillow or how the baby is held). Nursing an acrobatic toddler who may forget that he/she is breastfeeding when something more interesting comes by can cause pain.
Anatomical problems in the baby - There are anatomical issues other than tongue-tie or lip-tie that negatively impact breastfeeding. One of the most common is tight oral/neck musculature. This can stem from a traumatic birth, suboptimal intrauterine positioning, or torticollis. Congenital disorders of the baby can affect their oral or facial anatomy that can make breastfeeding extremely difficult (cleft lip or palate, for instance).
Specific factors affecting the breasts - While some of these factors can be caused by tongue-tie or lip-tie, diseases of the breasts themselves can be the sole cause of problems. Raynaud's disease or vasospasm can make breastfeeding extremely painful. Overly engorged breasts may make it difficult for the baby to latch on to a taut breast. Mastitis, plugged ducts, thrush and blebs can come from trauma during biting or chewing by the baby. Some moms have allergic reactions to products applied directly to the breasts (or to fragrances in toiletries or laundry). A small subset of moms have pain with letdown, or a painful milk ejection reflex. Others have severe negative emotions associated with letdown, called a dysphoric milk ejection reflex. A history of nipple piercings may have caused nerve sensitivity for mom during breastfeeding.
Psychological or other health factors that can affect breastfeeding - Postpartum depression can magnify any discomfort at the breast or can be interpreted as discomfort. This becomes especially apparent when the baby has other reasons to have breastfeeding problems (specifically with tongue-tie or lip-tie). Any history of sexual abuse can become a major hurdle for successful breastfeeding. Primary pain disorders like fibromyalgia can also become very problematic for a mom who is trying to nurse. Some moms experience increased discomfort when menstruation returns.
Equipment misuse - Improper use of a nipple shield can certainly cause problems breastfeeding, either leading to inefficiency of transfer, frustration for the baby or frank pain for mom. Additionally, improper use of a breast pump can cause undue pressure and pain on the nipples.
This list is by no means exhaustive. It is only meant to demonstrate that a mom who is experiencing difficulty with breastfeeding needs to visit someone who is versed in diagnosing these potential problems. Obviously, tongue-tie and lip-tie can play a role in breastfeeding problems, but I worry about the panacea-like mentality that can result when trying to solve a problem for a mom and baby. This is made even more likely given the desperation these dyads feel when something so basic and important becomes difficult.
February 20, 2014
by Bobby Ghaheri, Used with permission
As is the case with the identification of any new medical problem, there is bound to be excitement about helping those in need. Sometimes, that excitement can lead to false attribution of a problem to that "new" diagnosis. While tongue-tie or upper lip-tie are not technically new diagnoses, the correlation between tight frenula and breastfeeding problems is a relatively new one. Because I treat many babies each year where babies are having problems from tight frenula, I inevitably end up turning away many babies who aren't needing treatment.
Not every nail needs the same hammer. Tongue-tie and lip-tie may cause some, but not all, breastfeeding problems.
Not every nail needs the same hammer. Tongue-tie and lip-tie may cause some, but not all, breastfeeding problems.
The first place any mom and baby should go when breastfeeding problems arise is an IBCLC (international board certified lactation consultant). Here is a great post on how to choose a lactation consultant.
There are many potential causes of breastfeeding problems. I asked a group of great lactation consultants for a list of other causes for breastfeeding problems (specifically, pain). Here's what they came up with:
Technique problems - This includes poor latch technique, especially with positioning. Often, inexperienced moms picture breastfeeding like how a baby feeds from a bottle (this can also happen if the baby has nipple confusion when going from a bottle to the breast). They present the nipple instead of the breast, which can cause pain. Poor positioning can certainly be a problem (often caused by the wrong kind of pillow or how the baby is held). Nursing an acrobatic toddler who may forget that he/she is breastfeeding when something more interesting comes by can cause pain.
Anatomical problems in the baby - There are anatomical issues other than tongue-tie or lip-tie that negatively impact breastfeeding. One of the most common is tight oral/neck musculature. This can stem from a traumatic birth, suboptimal intrauterine positioning, or torticollis. Congenital disorders of the baby can affect their oral or facial anatomy that can make breastfeeding extremely difficult (cleft lip or palate, for instance).
Specific factors affecting the breasts - While some of these factors can be caused by tongue-tie or lip-tie, diseases of the breasts themselves can be the sole cause of problems. Raynaud's disease or vasospasm can make breastfeeding extremely painful. Overly engorged breasts may make it difficult for the baby to latch on to a taut breast. Mastitis, plugged ducts, thrush and blebs can come from trauma during biting or chewing by the baby. Some moms have allergic reactions to products applied directly to the breasts (or to fragrances in toiletries or laundry). A small subset of moms have pain with letdown, or a painful milk ejection reflex. Others have severe negative emotions associated with letdown, called a dysphoric milk ejection reflex. A history of nipple piercings may have caused nerve sensitivity for mom during breastfeeding.
Psychological or other health factors that can affect breastfeeding - Postpartum depression can magnify any discomfort at the breast or can be interpreted as discomfort. This becomes especially apparent when the baby has other reasons to have breastfeeding problems (specifically with tongue-tie or lip-tie). Any history of sexual abuse can become a major hurdle for successful breastfeeding. Primary pain disorders like fibromyalgia can also become very problematic for a mom who is trying to nurse. Some moms experience increased discomfort when menstruation returns.
Equipment misuse - Improper use of a nipple shield can certainly cause problems breastfeeding, either leading to inefficiency of transfer, frustration for the baby or frank pain for mom. Additionally, improper use of a breast pump can cause undue pressure and pain on the nipples.
This list is by no means exhaustive. It is only meant to demonstrate that a mom who is experiencing difficulty with breastfeeding needs to visit someone who is versed in diagnosing these potential problems. Obviously, tongue-tie and lip-tie can play a role in breastfeeding problems, but I worry about the panacea-like mentality that can result when trying to solve a problem for a mom and baby. This is made even more likely given the desperation these dyads feel when something so basic and important becomes difficult.
Resources
Once you start exploring the topic of tongue tie, you will find many helpful resources on the internet. Here are a few to get you started:
- https://www.facebook.com/groups/tonguetiebabies/ for mothers by mothers, this site has helped many parents through the process of discovering and resolving tongue tie.
- http://www.tonguetieclipit.com/Introduction.html
- http://www.cwgenna.com/ Catherine Watson Genna's site (author of Sucking Skills etc.)
- http://www.brianpalmerdds.com/ Dr. Brian Palmer's website
- http://www.kiddsteeth.com Dr. Kotlow's website
- http://www.tonguetie.net/ Speech Therapist Carmen Fernando's site
- http://massbreastfeeding.org/landscape/landscape.pdf Breastfeeding Helper Titles & What They Mean
- http://kellymom.com/health/baby-health/bfhelp-tonguetie/
- http://www.analyticalarmadillo.co.uk/2012/12/what-is-appropriate-aftercare-following.html
- https://drghaheri.squarespace.com/blog/2014/2/9/the-myths-about-painful-breastfeeding Article form Dr. Ghaheiri
- Dr. Bobby Ghaheri, Not All Breastfeeding Problems Are Caused by Tongue-Tie, drghaheri.com, http://www.drghaheri.com/blog/2014/2/20/not-all-breastfeeding-problems-are-caused-by-tongue-tiehttp:
- //thebreastfeedingmother.blogspot.com/2014/02/tongue-tie-and-low-weight-gain-tatums.html a mothers story
- Horsfall, Catherine (2013-05-31). Tongue tie: breastfeeding and beyond. A parents’ guide to diagnosis, division and aftercare. (Kindle Locations 5-7). Catherine Horsfall. Kindle Edition. A section on tongue tied bottlefeeding
- http://l.facebook.com/l/WAQEQIgb_AQEKC02A1Bv80AO3Vsd_05LrOdy8oLrll4tqhQ/www.ncbi.nlm.nih.gov/m/pubmed/24315215/ "CONCLUSIONS of the study: There was a statistically significant improvement in
speech outcomes and tongue mobility in children who underwent frenotomy compared to individuals who declined the operation. As a result of the data presented within this study, there appears to be a
long-term benefit beyond feeding when frenotomy is performed in newborns with ankyloglossia"
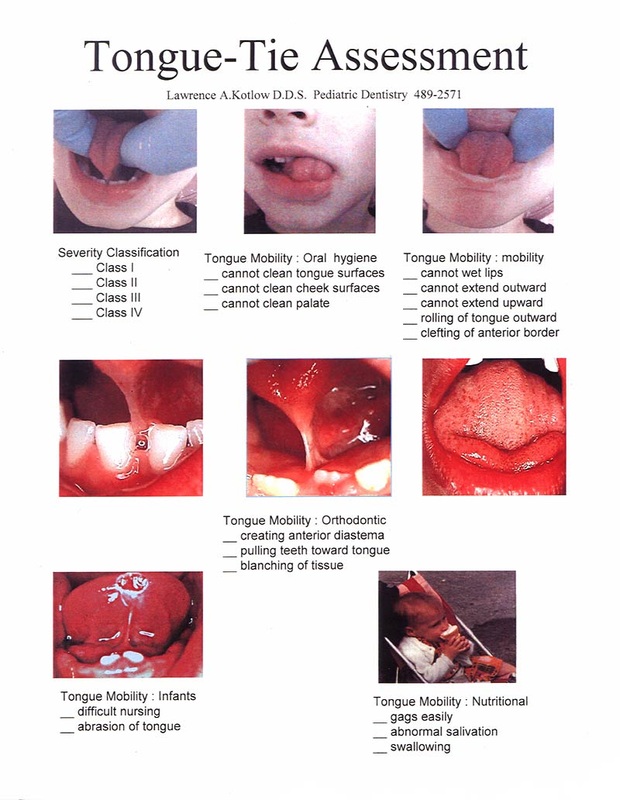
Tongue-Tie Assessment Sheet by Dr. Kotlow