Helping Babies who Have Down Syndrome Learn to Breastfeed
By J. Renee Toth

The breastfeeding experience is one of the first hands-on lessons that we as parents learn with our children. Sometimes these lessons do not come easily, as when our son with Down syndrome was born.
It took us eight months to arrive at a breastfeeding relationship. Now, when we breastfeed, I look at my baby and see him as a little boy. I forget that he has physical traits of Down syndrome because he’s just my son. He is my breastfed son.
In this article on breastfeeding a baby with Down syndrome, I would like to help mothers by providing a checklist of obstacles as well as solutions that have helped many mother-baby pairs. I will explore some of the common physical conditions our children have and their impact on breastfeeding, how swaddling and breastfeeding positions can help, as well as other aids and techniques.
You may also want to read articles on this website that concern breastfeeding: milk flow, milk supply, lactogenic foods and herbs.
It took us eight months to arrive at a breastfeeding relationship. Now, when we breastfeed, I look at my baby and see him as a little boy. I forget that he has physical traits of Down syndrome because he’s just my son. He is my breastfed son.
In this article on breastfeeding a baby with Down syndrome, I would like to help mothers by providing a checklist of obstacles as well as solutions that have helped many mother-baby pairs. I will explore some of the common physical conditions our children have and their impact on breastfeeding, how swaddling and breastfeeding positions can help, as well as other aids and techniques.
You may also want to read articles on this website that concern breastfeeding: milk flow, milk supply, lactogenic foods and herbs.
Mouth Feeding: An Opportunity to Develop a Basic Skill
Children who have Down syndrome learn differently than other children. Once we discover techniques that help, however, they can often learn the same things that come naturally to other babies and children.
In order to breastfeed effectively, our children need special lessons for increased muscle tone in the face, mouth, and tongue region, and for improved oral motor skills. They may need to be taught in a step-by-step fashion, and they need support until they are able to do things efficiently on their own.
The experience of mastering a basic skill such as mouth feeding can positively effect the child’s development for years to come. Unfortunately, many parents do not understand the far-reaching benefits of learning mouth-feeding skills, in particular for speech development. Remember, our children are capable of doing things that even just a decade ago no one thought possible. Medical advancement has come far recently as well, and the life expectancy of our children has risen from an average life span of 25 years to nearly 50.
In order to breastfeed effectively, our children need special lessons for increased muscle tone in the face, mouth, and tongue region, and for improved oral motor skills. They may need to be taught in a step-by-step fashion, and they need support until they are able to do things efficiently on their own.
The experience of mastering a basic skill such as mouth feeding can positively effect the child’s development for years to come. Unfortunately, many parents do not understand the far-reaching benefits of learning mouth-feeding skills, in particular for speech development. Remember, our children are capable of doing things that even just a decade ago no one thought possible. Medical advancement has come far recently as well, and the life expectancy of our children has risen from an average life span of 25 years to nearly 50.
Breastfeeeding Babies with Obstacles: A Longer Time-Line to Success
Many babies born with Down syndrome need surgeries in the early months, and may experience added obstacles that interfere with the energy and stamina needed to feed by mouth, whether at the bottle or on the breast.
Many mothers I’ve spoken to find that four to five months old is a turning point in their baby’s ability to breastfeed without as much support or guidance.
Just as every person, typical or not, learns at their own pace, it can take longer for some babies who have Down syndrome to learn to breastfeed. There are exceptions though, and breastfeeding can work from the early days and weeks without apparent difficulty.
There are special cases where direct breastfeeding has to be postponed: a baby’s medical diagnosis may require tube feedings; if breastmilk is necessary, alternative methods of feeding breastmilk are required. In the meantime, a mother can protect her milk supply by pumping and storing her breastmilk. When her baby is strong enough to take full feedings at the breast, the pumping mother will be able to nurse him.
Many mothers I’ve spoken to find that four to five months old is a turning point in their baby’s ability to breastfeed without as much support or guidance.
Just as every person, typical or not, learns at their own pace, it can take longer for some babies who have Down syndrome to learn to breastfeed. There are exceptions though, and breastfeeding can work from the early days and weeks without apparent difficulty.
There are special cases where direct breastfeeding has to be postponed: a baby’s medical diagnosis may require tube feedings; if breastmilk is necessary, alternative methods of feeding breastmilk are required. In the meantime, a mother can protect her milk supply by pumping and storing her breastmilk. When her baby is strong enough to take full feedings at the breast, the pumping mother will be able to nurse him.
Signs and Symptoms of Common Challenges
The symptoms listed here are intended only as a checklist. They are not present in all children who have Down syndrome, and they can range from very mild to very severe.
1. Low Muscle Tone
Low muscle tone, also known as hypotonia, can present itself with “floppy” limbs, head, and a protruding tongue. It can also be described as the baby feeling like a “rag doll” easily slipping through an adult’s grasp. Physical Therapy (PT) will help develop your baby’s overall muscle tone.
Our babies who have low tone may also have swallow dysfunctions, and require oral motor therapy to gain the skills needed to feed effectively at the breast or the bottle. The expert to look to for help is a Speech Pathologist who is trained in feeding issues and oral motor therapy in children who have Down syndrome. As the baby develops muscle strength and gains coordination with Physical Therapy (PT) and Occupational Therapy (OT), you’ll start to see important milestones, such as correct latch and effective drinking coordination in your baby.
Recognizing Hypotonia of the Mouth Region in Babies with Down Syndrome:
Our babies who have low tone may also have swallow dysfunctions, and require oral motor therapy to gain the skills needed to feed effectively at the breast or the bottle. The expert to look to for help is a Speech Pathologist who is trained in feeding issues and oral motor therapy in children who have Down syndrome. As the baby develops muscle strength and gains coordination with Physical Therapy (PT) and Occupational Therapy (OT), you’ll start to see important milestones, such as correct latch and effective drinking coordination in your baby.
Recognizing Hypotonia of the Mouth Region in Babies with Down Syndrome:
- Baby sucks badly or not at all from the breast
- Bottle drinking is difficult or not possible
- Baby may not be able to make an adequate vacuum (there could be a gap in the corner of his/her mouth/lips)
- Some babies with hypotonia do not have a sucking reflex, or a decreased one
- The rooting reflex is sometimes missing
- Weight loss will happen if the infant’s feeding problem remains undiscovered (Sleepy babies who do not always wake to eat or who spend time at the breast not getting sufficient quantities of milk.)
- The philtrum (area between the upper lip and nose) looks flatter than that of typical strong newborns
- Facial muscles may be less active than typical strong newborns (diminished facial expressions)
- Low muscle tone elsewhere, “floppy” limbs
- Baby smiles less or not at all
2. Non-Rhythmic Suck
Due to lack of coordination, some babies have a unique sucking sequence. Most mothers who have previously had a breastfeeding baby will notice the difference. Weak reflexes for sucking and swallowing can present as gagging and coughing during a feeding. This can be a sign of a confused suck, swallow, and breathing process such as Dysphagia or aspiration of liquid , and may require a professional such as a Speech Pathologist trained in infant feeding problems. This too will improve as baby gains strength with ongoing PT and OT.
3. Arching
Arching backwards can be caused by low muscle tone, though it is also frequently impacted by GERD-reflux (below). In cases of low muscle tone, these babies can often be helped by swaddling, described later in this article. The baby may also be more comfortable nursing in a more upright and well-supported position.
Babies with low muscle tone will often brace their feet against objects, such as the arm of a chair or sofa, in an effort to stabilize themselves. This in turn leads to arching. Providing your baby with physical support in a comfortable position can reduce their need to do this. Swaddling often does the trick. You may also want to think about your seating, and sit in an open chair rather than a chair that allows your baby to resume feet-bracing and arching.
Using gravity well in supporting a baby can make nursing more comfortable. For instance, the so-called Australian position, where the mother is reclined on her back, and the baby is lying face down on her breasts.
Babies with low muscle tone will often brace their feet against objects, such as the arm of a chair or sofa, in an effort to stabilize themselves. This in turn leads to arching. Providing your baby with physical support in a comfortable position can reduce their need to do this. Swaddling often does the trick. You may also want to think about your seating, and sit in an open chair rather than a chair that allows your baby to resume feet-bracing and arching.
Using gravity well in supporting a baby can make nursing more comfortable. For instance, the so-called Australian position, where the mother is reclined on her back, and the baby is lying face down on her breasts.
4. Gastro Esophageal Reflux Disease (GERD)
Gastro Esophageal Reflux Disease, also known as GERD or reflux, is another common reason for arching. It is very common in children who have Down syndrome due to low muscle tone in the trunk, trachea, and esophagus. GERD can present itself very clearly as vomiting, or in the “silent form” with arching while gulping, coughing while feeding, and an “erp’ing” sound in the back of the throat. Drooling is also common as the saliva builds up in his mouth and he tries to avoid swallowing. When babies experience pain because of untreated reflux, they may eventually refuse the source of the pain -- the breast! This is called breast refusal.
While there are other reasons for arching, such as neurological, it is worth getting this checked first since it is so common and because reflux is a health hazard for a baby. Untreated, reflux can cause erosion of the esophagus by stomach acid that is brought up during a reflux episode. Also, if the child aspirates thin liquids into the lungs, which can be determined with a swallow study, they are more prone to respiratory problems that can lead to pneumonia.
Refusal to feed because of the association of pain can be a very hard process for both the mother and baby. As with reflux, if a baby associates aspiration with feeding at the breast, he can start to refuse the source of pain, the breast.
Breastfeeding positions can help the baby control the amount of milk they suck; a smaller amount reduces the symptoms of reflux. As well, there are several alternative options for providing breastmilk to a baby with aspiration challenges.
GERD can be set off by something the mother eats. By keeping a diary of what she eats and drinks, many mothers discover “trigger foods” to eliminate from their diet, and the baby’s reflux improves. The baby may also be given a medication if needed.
While there are other reasons for arching, such as neurological, it is worth getting this checked first since it is so common and because reflux is a health hazard for a baby. Untreated, reflux can cause erosion of the esophagus by stomach acid that is brought up during a reflux episode. Also, if the child aspirates thin liquids into the lungs, which can be determined with a swallow study, they are more prone to respiratory problems that can lead to pneumonia.
Refusal to feed because of the association of pain can be a very hard process for both the mother and baby. As with reflux, if a baby associates aspiration with feeding at the breast, he can start to refuse the source of pain, the breast.
Breastfeeding positions can help the baby control the amount of milk they suck; a smaller amount reduces the symptoms of reflux. As well, there are several alternative options for providing breastmilk to a baby with aspiration challenges.
GERD can be set off by something the mother eats. By keeping a diary of what she eats and drinks, many mothers discover “trigger foods” to eliminate from their diet, and the baby’s reflux improves. The baby may also be given a medication if needed.
5. Aspiration
As mentioned above, if the child aspirates thin liquids into the lungs, which can be determined with a swallow study, they are more prone to respiratory problems that can lead to pneumonia. If they aspirate enough fluid into their lungs they have a life-threatening situation. An alternative feeding method such as thickened breastmilk fed by finger feeding or bottle feeding may be what is needed. A swallow study will determine how thick the liquid needs to be for the child's specific swallow dysfunction. There are special commercial thickeners that can be added to breastmilk (or any liquid) to a nectar or honey consistency depending on the child's diagnosis.
Sometimes, a baby cannot feed from the breast or bottle due to the danger of aspiration while feeding, and a feeding tube may be necessary. Some babies only need them for a short period of time. Aspiration problems can be helped with oral motor therapy by a trained Speech Pathologist trained in treating babies with swallow problems.
Thickeners: Breastmilk can be thickened with a commercial thickener such as Simply Thick® gel to either Nectar or Honey consistency. This reduces the danger of aspiration. Use stage three nipples or cross-cut nipples to enable the baby to drink thickened milk. “Simply Thick®” can be ordered or bought through a pharmacy or online.
Sometimes, a baby cannot feed from the breast or bottle due to the danger of aspiration while feeding, and a feeding tube may be necessary. Some babies only need them for a short period of time. Aspiration problems can be helped with oral motor therapy by a trained Speech Pathologist trained in treating babies with swallow problems.
Thickeners: Breastmilk can be thickened with a commercial thickener such as Simply Thick® gel to either Nectar or Honey consistency. This reduces the danger of aspiration. Use stage three nipples or cross-cut nipples to enable the baby to drink thickened milk. “Simply Thick®” can be ordered or bought through a pharmacy or online.
6. Over or Under-Sensitive to Stimulation
This is common for babies who have Down syndrome. Some babies respond better and nurse for longer periods of time in a dark, quiet environment where they can concentrate fully on the task at hand. Other babies respond better to loud, exciting music with a bouncy beat and being pat on the back to help keep them stimulated and awake during a feeding.
7. Sleepy Babies
Our babies tend to be sleepy and to fall asleep at the breast before they get a chance to get the hindmilk – the creamy, calorie-rich milk that comes later in a feed, and that is important to a baby’s neural development and weightgain.
Babies with congenital heart defects can have an especially challenging time having enough energy to get hindmilk. Pre-pumping the foremilk, or expressing until a letdown begins, can help the baby use less energy to start the flow of milk. This will allow them to use their energy to drink the milk that is already flowing and to get the hindmilk before tiring out.
While sleepiness may be related to our baby’s special issues such as heart problems, all babies can be sleepy as a way of “checking out” at the breast.
Beverly Morgan IBCLC notes that, “A baby who is overwhelmed or overstressed may just check out for a snooze. This shut down mode can help him cope. If the baby is awake when mothers starts feeding, but goes to sleep immediately or very soon, she can try changing something about the feeding situation. For instance, a dark or a light room, turning off music or turning it on, not rocking when nursing, or adding in a rocking motion, swaddling the baby or unswaddling the baby, holding the baby upright, or laying him on the mother’s chest while she is laying on her back. The baby’s reactions will help a mother discover just what works best for her baby. A baby that is sleepy or squirmy or a pokey eater may be less so when he is comfortable.”
Often, our sleepy babies do not “cue” when they are hungry and the mother may need to take a more scheduled approach. It may be necessary to wake and rouse the baby to breastfeed every 2 to 2 ½ hours if they show no interest or signs of hunger before then. Breastfeeding a baby with Down syndrome “on demand” often needs to be saved for later when the child is able to cue and is not as sleepy.
A Breast Pump can Help Baby and Mother
Pre-pumping the foremilk, or expressing until a letdown begins, can help sleepy babies use less energy to start the flow of milk. This will allow them to use their energy to drink the milk that is already flowing and to get the hindmilk before tiring out.
Pumping after a feeding and feeding it to the baby in a bottle, or freezing it (marked carefully as hindmilk), is a strategy to help a baby gain weight, and to keep a mother’s milk supply ample.
Babies with congenital heart defects can have an especially challenging time having enough energy to get hindmilk. Pre-pumping the foremilk, or expressing until a letdown begins, can help the baby use less energy to start the flow of milk. This will allow them to use their energy to drink the milk that is already flowing and to get the hindmilk before tiring out.
While sleepiness may be related to our baby’s special issues such as heart problems, all babies can be sleepy as a way of “checking out” at the breast.
Beverly Morgan IBCLC notes that, “A baby who is overwhelmed or overstressed may just check out for a snooze. This shut down mode can help him cope. If the baby is awake when mothers starts feeding, but goes to sleep immediately or very soon, she can try changing something about the feeding situation. For instance, a dark or a light room, turning off music or turning it on, not rocking when nursing, or adding in a rocking motion, swaddling the baby or unswaddling the baby, holding the baby upright, or laying him on the mother’s chest while she is laying on her back. The baby’s reactions will help a mother discover just what works best for her baby. A baby that is sleepy or squirmy or a pokey eater may be less so when he is comfortable.”
Often, our sleepy babies do not “cue” when they are hungry and the mother may need to take a more scheduled approach. It may be necessary to wake and rouse the baby to breastfeed every 2 to 2 ½ hours if they show no interest or signs of hunger before then. Breastfeeding a baby with Down syndrome “on demand” often needs to be saved for later when the child is able to cue and is not as sleepy.
A Breast Pump can Help Baby and Mother
Pre-pumping the foremilk, or expressing until a letdown begins, can help sleepy babies use less energy to start the flow of milk. This will allow them to use their energy to drink the milk that is already flowing and to get the hindmilk before tiring out.
Pumping after a feeding and feeding it to the baby in a bottle, or freezing it (marked carefully as hindmilk), is a strategy to help a baby gain weight, and to keep a mother’s milk supply ample.
8. Milk Flow
All babies have a preference for milk flow, faster or slower. Breast compression can help increase the speed of milk flow, and the so-called “scissors hold” can slow the flow. Remember, babies with reflux and with swallow issues will probably want a slower flow.
Breastfeeding Positions and Aids for Specific Problems
Positioning our babies with low muscle tone is an important key to latching on, and to the length of time that the baby has energy to feed. This in turn affects the mother’s milk supply, and sets the stage for a happy, successful relationship to develop. There are many breastfeeding positions that may be best for your child, some more conventional than others. See an IBCLC for help finding the positions that are best for your baby.
1. Swaddling for Low Muscle Tone

If the baby with low muscle tone is not in a good position, or is not receiving enough body support, it can take much longer to complete a feeding, both with a bottle or breast. Swaddling has been shown to help our babies feed by mouth faster if they have low energy levels or seem to spend much of their time trying to hold up their loose bodies.
It is hard to describe holding a baby who has low muscle tone. If you hold the child out in front of you to coo at them, their arms will hang down unnaturally toward the floor. They have very loose joints and ligaments. When being held, in the cradle hold for instance, their arms can easily get wrapped up behind them literally resting their wrist on their spine while the shoulder is twisted up. They don’t show any pain with these rubber band antics. Just holding a baby with low tone is very difficult.
Swaddling can give this baby needed support, and can make it possible for the mother to properly position and latch on her baby. I’ll go into more detail about swaddling a low tone baby, but first, I’d like to discuss our personal story.
Before we learned an appropriate swaddling technique and my son was learning to drink by mouth, (from a bottle while weaning off of a feeding tube), I had to support his jaw against the bottle and rock and pat him since he was one of the easily "under-stimulated" babies. He also had three holes in his heart making his energy levels low; sucking alone wore him out. I was lucky that he preferred to taste his milk rather than being fed directly into his stomach with a tube. However, trying to keep his mouth latched onto the bottle, and trying to hold up his limp body limbs, as well as dealing with his tendency to arch from reflux and low tone was time consuming and frustrating. Without swaddling, feeding could take a long time: three straight hours to drink three ounces from a bottle. Just in time to start another three ounces. This left little time for pumping or caring for the rest of my family.
Once we discovered the swaddling position described below he IMMEDIATELY was able to take a feeding of three ounces in 1/2 hour. I cried for joy the first time this happened. The difference was so dramatic. In talking with other mothers who use this technique, I found it was helpful for many of them, too. However, it will not be the best technique for all babies. Remember that these are only suggestions, and that only your experience with your baby will prove what is best and right for her.
How to Swaddle a Baby with Low Muscle Tone
Swaddle your baby in a baby blanket. Cross her arms over her chest, and cross her legs while pulling her knees to her chest. Then swaddle snugly. Swaddling can be used in any feeding position that you have found is good for your baby. It can be helpful for many months past when a mother of a baby with average tone would have stopped swaddling. Swaddling materials can be made quickly and inexpensively for older babies by using a larger piece of fabric.
Swaddling is not always the answer. Sometimes the baby instantly falls asleep while swaddled instead of staying alert to feed. With babies who have low tone and who are not clear with their cues, it is especially important for parents to watch the baby’s cues that he is comfortable. Some babies may prefer to have their arms free, or to be swaddled more loosely.
It is hard to describe holding a baby who has low muscle tone. If you hold the child out in front of you to coo at them, their arms will hang down unnaturally toward the floor. They have very loose joints and ligaments. When being held, in the cradle hold for instance, their arms can easily get wrapped up behind them literally resting their wrist on their spine while the shoulder is twisted up. They don’t show any pain with these rubber band antics. Just holding a baby with low tone is very difficult.
Swaddling can give this baby needed support, and can make it possible for the mother to properly position and latch on her baby. I’ll go into more detail about swaddling a low tone baby, but first, I’d like to discuss our personal story.
Before we learned an appropriate swaddling technique and my son was learning to drink by mouth, (from a bottle while weaning off of a feeding tube), I had to support his jaw against the bottle and rock and pat him since he was one of the easily "under-stimulated" babies. He also had three holes in his heart making his energy levels low; sucking alone wore him out. I was lucky that he preferred to taste his milk rather than being fed directly into his stomach with a tube. However, trying to keep his mouth latched onto the bottle, and trying to hold up his limp body limbs, as well as dealing with his tendency to arch from reflux and low tone was time consuming and frustrating. Without swaddling, feeding could take a long time: three straight hours to drink three ounces from a bottle. Just in time to start another three ounces. This left little time for pumping or caring for the rest of my family.
Once we discovered the swaddling position described below he IMMEDIATELY was able to take a feeding of three ounces in 1/2 hour. I cried for joy the first time this happened. The difference was so dramatic. In talking with other mothers who use this technique, I found it was helpful for many of them, too. However, it will not be the best technique for all babies. Remember that these are only suggestions, and that only your experience with your baby will prove what is best and right for her.
How to Swaddle a Baby with Low Muscle Tone
Swaddle your baby in a baby blanket. Cross her arms over her chest, and cross her legs while pulling her knees to her chest. Then swaddle snugly. Swaddling can be used in any feeding position that you have found is good for your baby. It can be helpful for many months past when a mother of a baby with average tone would have stopped swaddling. Swaddling materials can be made quickly and inexpensively for older babies by using a larger piece of fabric.
Swaddling is not always the answer. Sometimes the baby instantly falls asleep while swaddled instead of staying alert to feed. With babies who have low tone and who are not clear with their cues, it is especially important for parents to watch the baby’s cues that he is comfortable. Some babies may prefer to have their arms free, or to be swaddled more loosely.
2. Low Mouth Tone: Dancer Hand Position
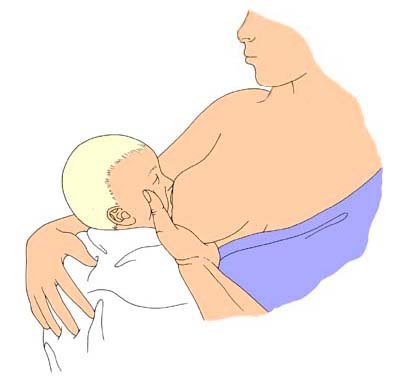
This jaw support can be used with mouth feedings, breast or bottle, to aid in proper. To support the baby’s bottom jaw, the mother slides her hand beneath her breast and forward, so she is supporting the breast with three fingers rather than four. She forms a U-shape with her thumb and forefinger to cradle her baby’s chin. This will help the baby press the nipple and areola between the gums. Now comes the tricky part. While the U-form between the thumb and first finger holds the baby’s bottom jaw up against the nipple, the same thumb and finger gently and firmly squeeze the baby’s cheeks together until the entire mouth forms a seal on the nipple. This can be done while breastfeeding or feeding with a bottle.
3. GERD-Reflux: Mother Reclining with Baby Face Down (so-called “Australian Position”)

This position helps with GERD, with swallow/suck/breathe coordination (more control over milk flow), and with achieving a better suction/seal in mouth region. The baby uses less energy holding her body and can relax her muscles against mother with much more full body support. Remember to keep baby’s nose free to breathe!
4. Alternative Feeding Methods

Talk to your IBCLC and OT to discuss which alternative feeding method is appropriate for your baby: Nipple Shield; Supplemental Nursing System™ (SNS™) or Lact-Aid®; medicine cup (feeding baby straight from a cup); finger feeding; Haberman™ Feeder; bottle; feeding tubes (G-tube or NG tube).
5. Side Laying

Mother and baby face tummy to tummy on a comfortable surface. Using a pillow under mother’s head, behind her back, and behind baby’s back is helpful for full support and good seal and latch.
6. Football Hold

Think about how you cradle a football beneath your arm when you run with it. As a breastfeeding position, the baby’s body also lays beneath the mother’s arm. Use pillows or a nursing pillow as support for the baby’s body. As the baby latches on to the breast, her shoulders are under your arm, and her body is wrapped around toward your back.
7. Cradle Hold with the Baby’s Head Higher than his Body

In this classic position, holding the head higher that his body is a good option for babies with low tone who have these common problems: reflux, swallow dysfunction, and/or weak latch. The mother can prop her elbows as needed to keep her baby’s head up high.
Conclusion
Today, when I hold my child against me and look into his beautiful eyes, I take nothing for granted. He and I were able to overcome more obstacles than I ever knew were possible. I pumped his milk for eight months so that he could feed by feeding tube, or receive my milk thickened in a bottle. He finally gained the strength and coordination to feed fully at the breast! Now that we are well past his first birthday, breastfeeding is still a young experience that we both hold on to tightly.
I know that not all mothers and babies with Down syndrome share our struggle; many have an easy time right from the start. There are also mothers and babies who never reach their goal to breastfeed.
Take heart. Breastfeeding or breastmilk is not the only thing that makes a mother the most important person in a baby’s life. Babies need more than breastmilk. They need love, guidance, nurturing, and all the other wonderful things that we can provide regardless of whether we are able to feed them at the breast. Please remember that your babies love you for all of you and for all that you provide for them!
I know that not all mothers and babies with Down syndrome share our struggle; many have an easy time right from the start. There are also mothers and babies who never reach their goal to breastfeed.
Take heart. Breastfeeding or breastmilk is not the only thing that makes a mother the most important person in a baby’s life. Babies need more than breastmilk. They need love, guidance, nurturing, and all the other wonderful things that we can provide regardless of whether we are able to feed them at the breast. Please remember that your babies love you for all of you and for all that you provide for them!